
Texas Medicaid Provider Enrollment Transformation FrameworkTransforming a Legacy Healthcare Enrollment System Without Replacing It
How might we reduce errors, rework, and operational inefficiencies in a complex Medicaid enrollment system while laying the foundation for future automation and AI-enabled support?
Texas Medicaid's provider enrollment process was one of the most complex administrative systems in the United States. Providers regularly struggled to navigate enrollment requirements, while processors, support teams, and policy stakeholders relied on disconnected information sources, creating costly delays, rework, and frustration.
The system itself could not be replaced. Any improvements had to work within existing technological, operational, and regulatory constraints.
The Challenge
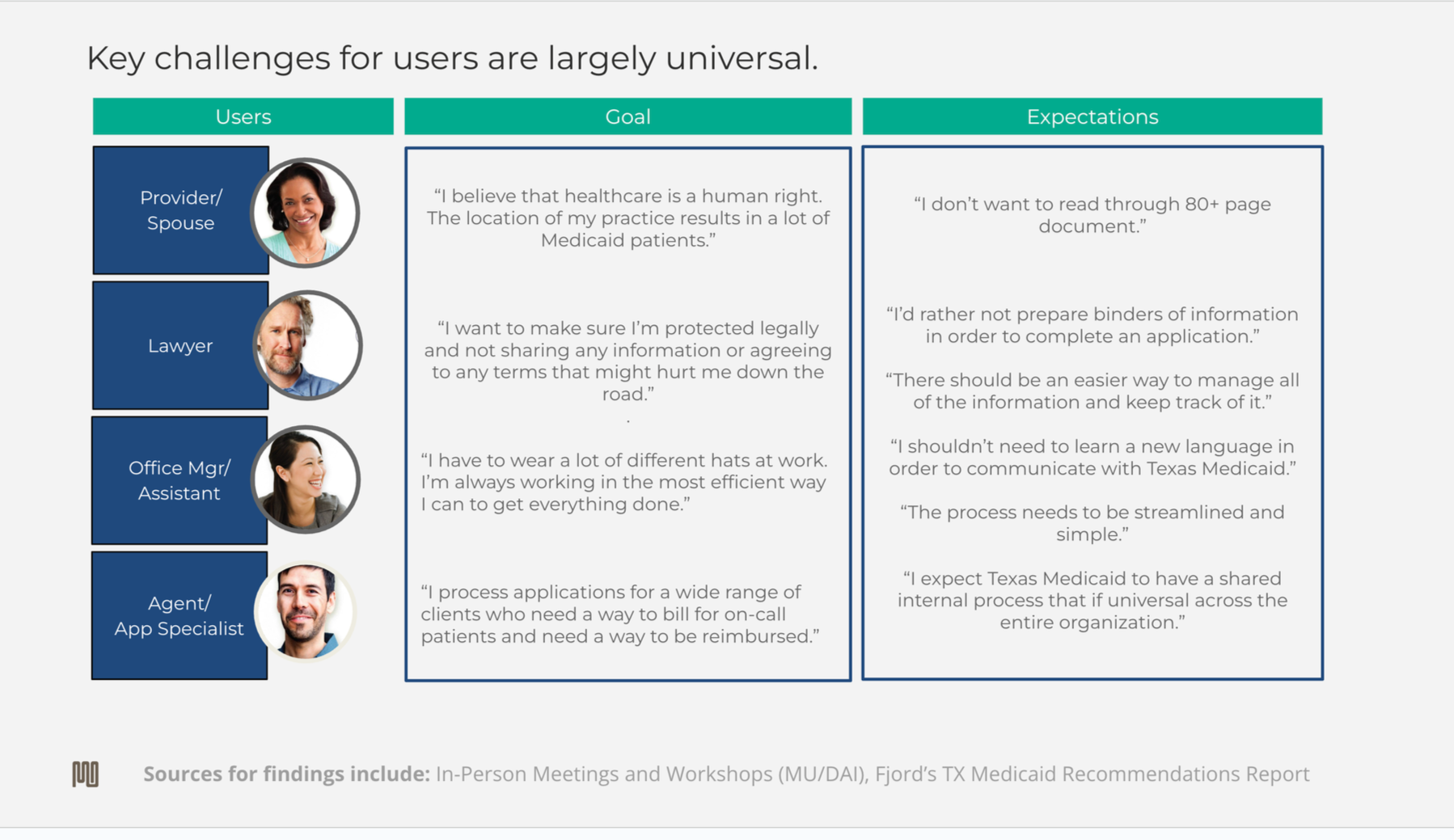
The Texas Medicaid Provider Enrollment process required providers to navigate a highly specialized regulatory environment using terminology, classifications, and policy language that often differed from how providers understood their own businesses.
As a result, many providers relied on third-party enrollment specialists to complete applications successfully. The enrollment process had become less about understanding healthcare eligibility requirements and more about understanding how to interpret the system itself.
Compounding the problem, enrollment errors were difficult to unwind. Because Medicaid operates within a highly regulated environment, submitted information becomes part of the permanent administrative record. Incorrect submissions often triggered lengthy correction cycles, additional reviews, support calls, and operational delays.
The challenge was not simply reducing user error.
The challenge was helping providers make correct decisions before information entered the system.
What I Did
Conducted Field Research
Observed processors entering paper applications into the legacy enrollment system and documented:
Error patterns
Policy interpretation challenges
Escalation triggers
Decision-making behaviors
Conducted interviews with:
Enrollment processors
Quality assurance teams
Contact center agents
Policy stakeholders
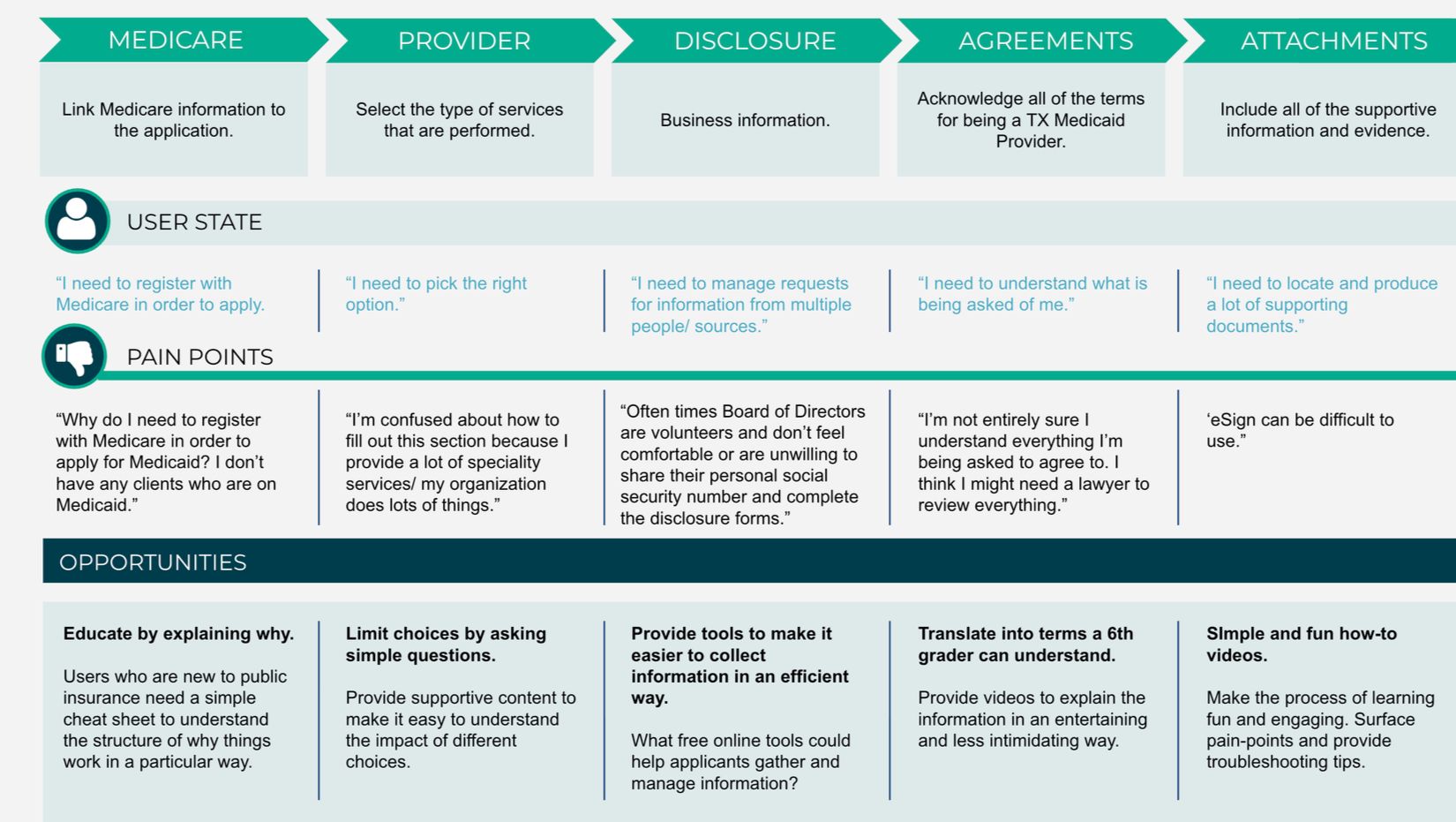
Mapped Systemic Failure Points
Created journey maps and workflow models showing:
Provider confusion points
Processor interpretation gaps
Rework loops
Escalation pathways
Knowledge bottlenecks
Identified how content ambiguity created operational inefficiencies throughout the enrollment ecosystem.
Analyzed Operational Performance Data
Reviewed enrollment performance metrics including:
Contact center resolution times
Application rejection rates
Rework frequency
Escalation patterns
Processing delays
Connected qualitative research findings to measurable operational outcomes.
Reframed Information Architecture as Infrastructure
Designed a content governance and information architecture framework that:
Established ownership models
Introduced review and maintenance processes
Organized content around user tasks and provider types
Reduced conflicting guidance across channels
Created foundations for future knowledge retrieval systems
Designed Decision Support Tools
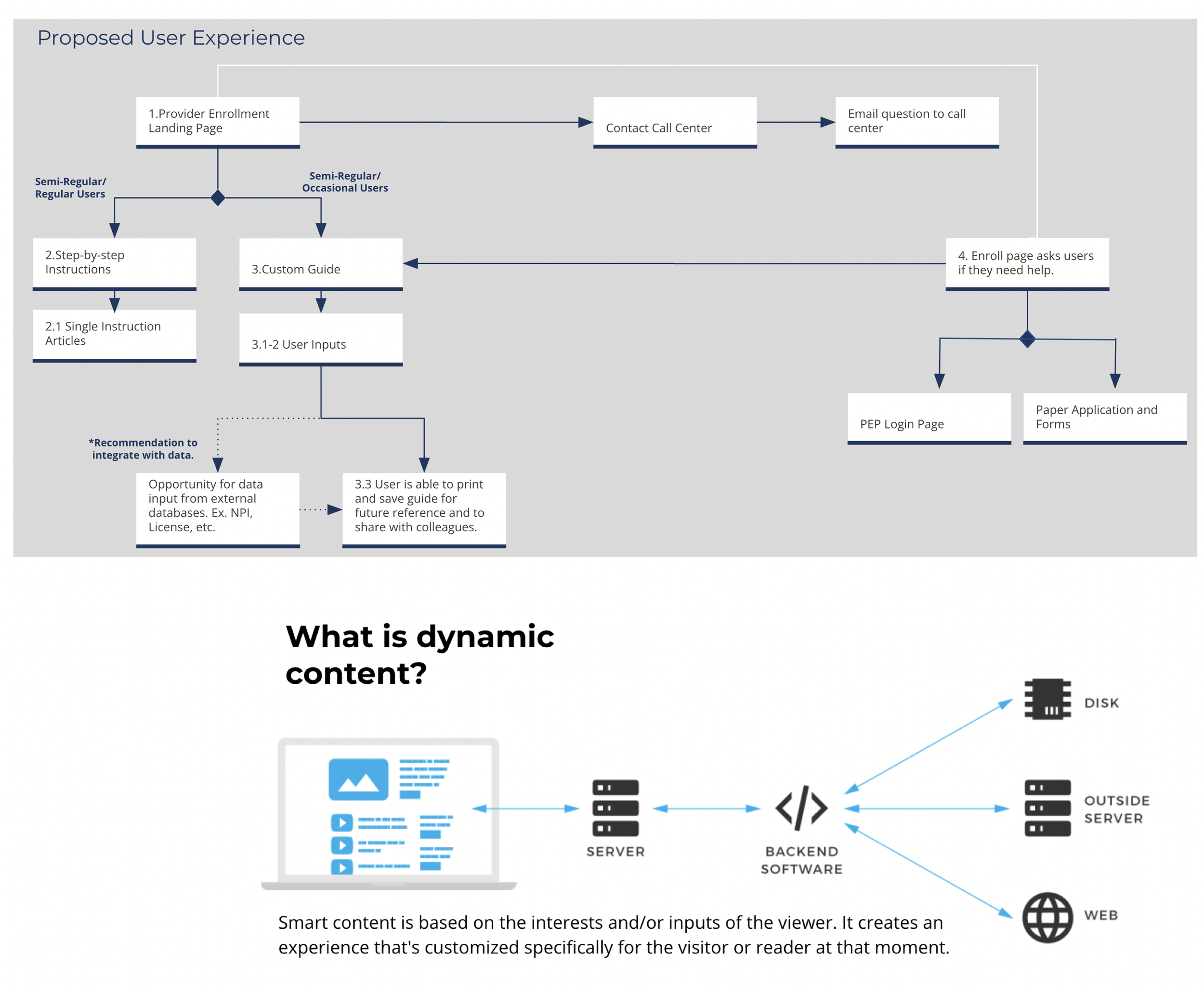
Prototyped a guided support experience that:
Asked providers logic-based questions
Personalized enrollment guidance
Reduced cognitive load
Directed users toward relevant forms and requirements
The solution demonstrated how simple decision-support mechanisms could significantly reduce downstream errors.

Key Deliverables
Operational Workflow Analysis
End-to-end mapping of provider enrollment workflows, processor activities, and escalation pathways.
Content Governance Framework
Governance model defining content ownership, maintenance processes, and policy alignment mechanisms.
Information Architecture & Taxonomy
Task-based information structure supporting consistency across channels and future knowledge systems.
Guided Enrollment Decision Support Prototype
An interactive logic-based support tool that dynamically tailors enrollment guidance to provider needs.
Operational Performance Analysis
Research-backed analysis linking content ambiguity and process failures to measurable operational costs.
Executive Transformation Roadmap
Strategic recommendations balancing immediate operational improvements with long-term modernization goals.
Why This Work Matters
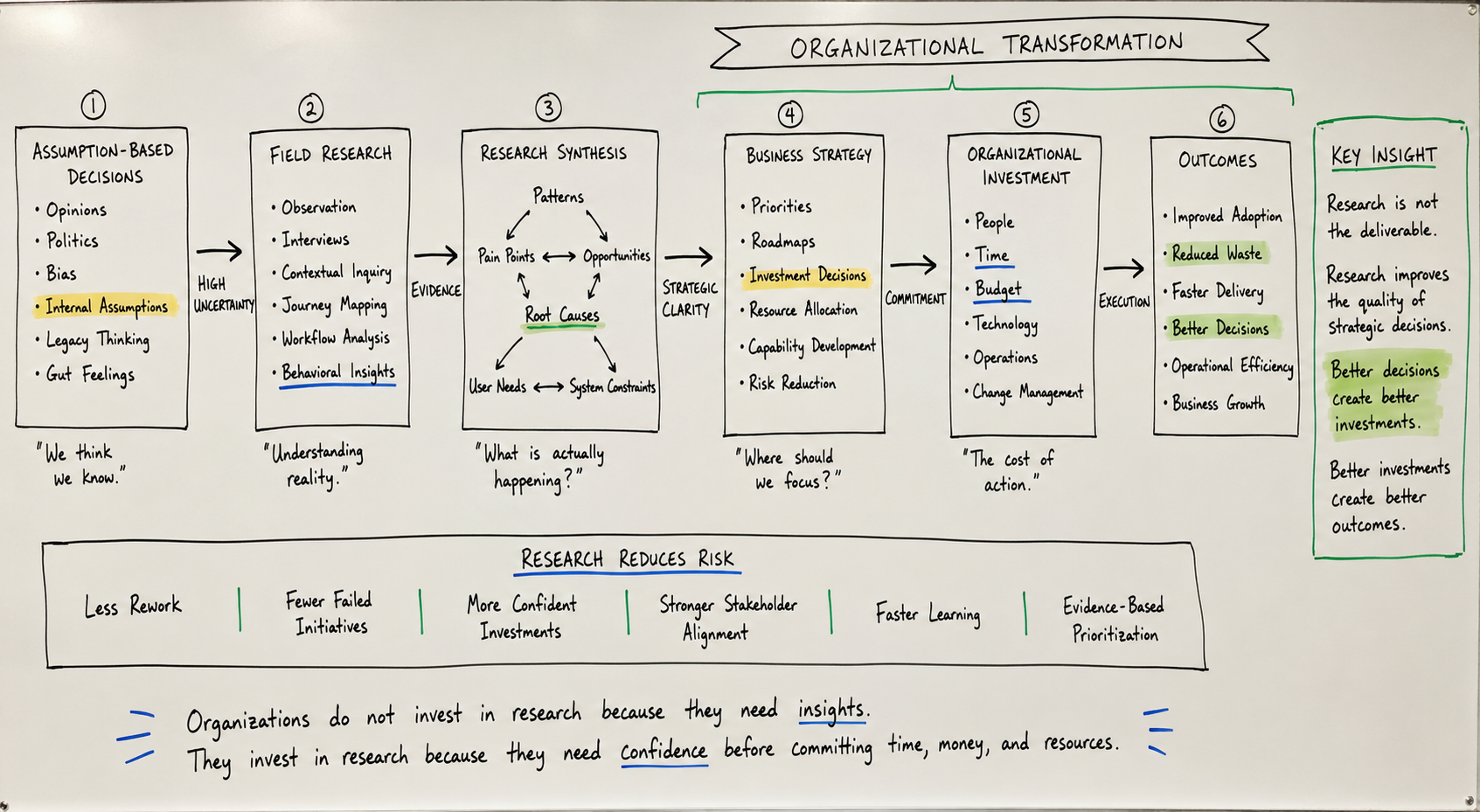
This project revealed an important lesson that extends far beyond healthcare. Many organizations assume users fail because they need more training. In reality, people often fail because systems require them to adopt unfamiliar mental models, terminology, and decision frameworks without sufficient support.
The Medicaid enrollment process had unintentionally created a dependency on human intermediaries whose primary value was translating complexity. The work demonstrated that effective transformation begins by reducing ambiguity at the point of decision-making.
By introducing a clearer information architecture, content governance, and guided decision support, the project demonstrated how organizations can reduce errors before they occur rather than managing their consequences afterward.
The implications extend directly to AI and automation initiatives today. AI systems cannot compensate for unclear terminology, fragmented knowledge, or inconsistent governance. Before organizations can automate decisions, they must first create a shared understanding. In that sense, this project was not simply about enrollment. It was about designing systems that help humans make better decisions in complex environments. That's the same challenge organizations face today as they prepare for AI-assisted work.
KEY INSIGHT
The enrollment system was designed around Medicaid's language, not the provider's language.
Providers were being asked to translate their businesses into a complex regulatory framework with limited guidance and little support.
Many errors occurred not because users lacked knowledge, but because the system lacked mechanisms to help users interpret policy, terminology, and requirements in context.
This reframed the problem:
The system did not need more instructions. It needed translation, guidance, and decision support.
Problem Context
Texas Medicaid’s provider enrollment process is among the most complex in the United States. At the time of this engagement, enrollment was largely paper-based, policy-dense, and manually processed, even for experienced providers. Many healthcare providers hired third-party specialists simply to navigate the application correctly TX Medicaid Provider Enrollment.
Applications were submitted on paper and manually entered into a legacy system by Accenture staff. This introduced error at multiple points:
providers misinterpreting forms or submit incomplete information
processors inconsistently interpreting policies during data entry
applications cycling through months of rejection and rework
call centers overwhelmed by clarification requests and escalations TX Medicaid Provider Enrollment…
Critically, there was no central source of truth:
provider-facing instructions conflicted across web pages, PDFs, and call scripts
internal processor documentation had no ownership model or review cycle
“shadow guidance” emerged informally, creating systemic inconsistency TX Medicaid Provider Enrollment…
Design Constraint
This was a constraint-heavy environment:
legacy infrastructure could not be replaced
digital research tooling did not yet exist
automation was not feasible in the short term
recommendations had to work within the existing system
The design challenge was therefore not “how do we redesign the system,” but:
How do we reduce error, confusion, and rework now, while creating a foundation for future automation later?
Research Approach
I used a mixed-methods, immersive research approach to understand how the system actually operated across roles, not how it was documented.

This space served as both a synthesis mechanism and a collaborative artifact, fostering alignment and trust among policy, processing, and support teams.
Methods
Shadowed Accenture processors entering paper applications into the legacy system, documenting error patterns, decision fatigue, and policy ambiguity
Conducted contextual interviews with processors and QA leads
Facilitated cognitive walkthroughs with contact center agents using real support calls
Reviewed, rejected, and escalated application packets to identify systemic patterns
Mapped provider and processor journeys to surface rework loops and friction points
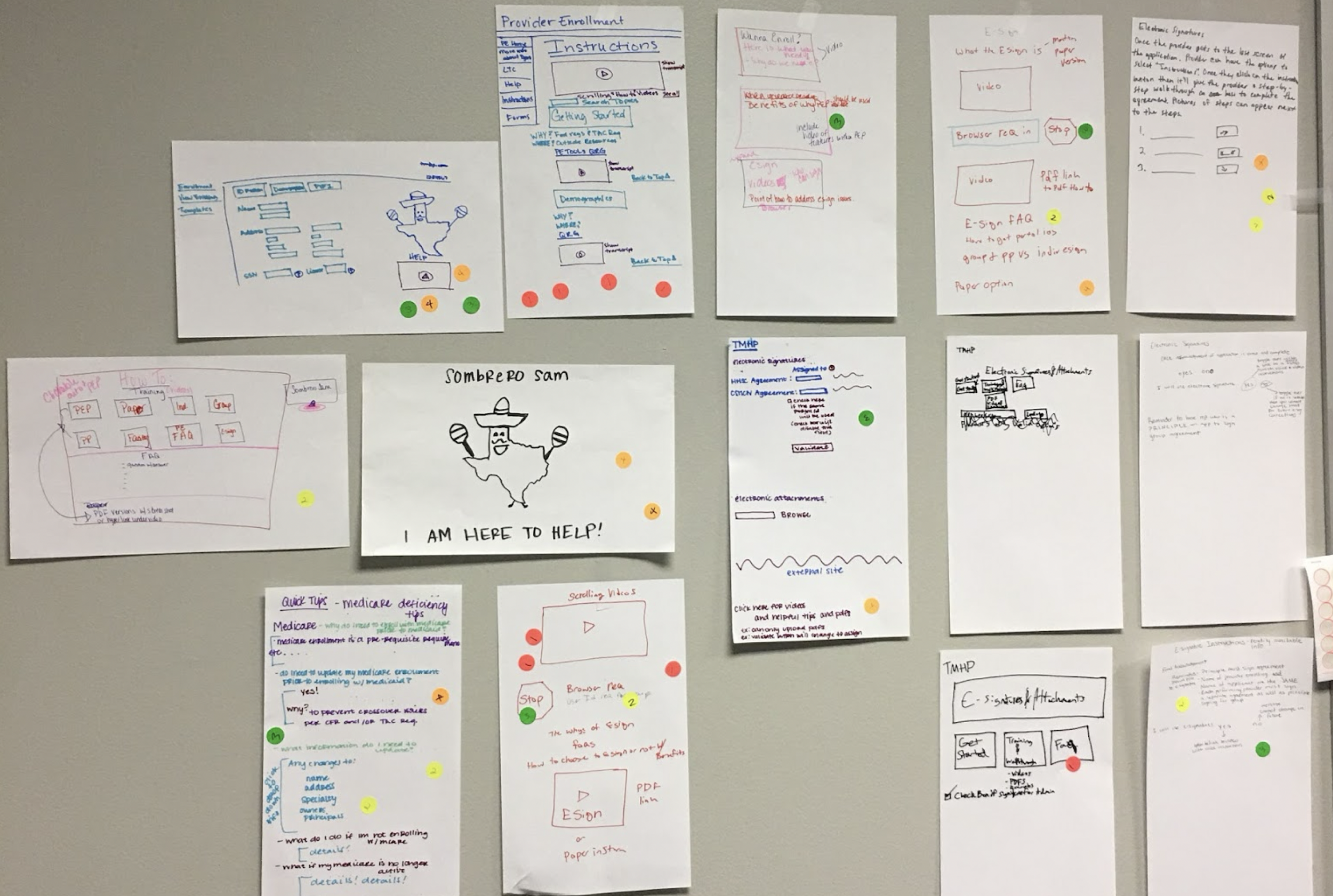
I created a physical “research war room” at the TMHP office:
manually transcribed interview notes, quotes, and form analysis onto Post-its
used affinity mapping and color-coded clustering to surface recurring breakdowns
invited TMHP stakeholders to walk the room with me, validating patterns and assumptions in real time
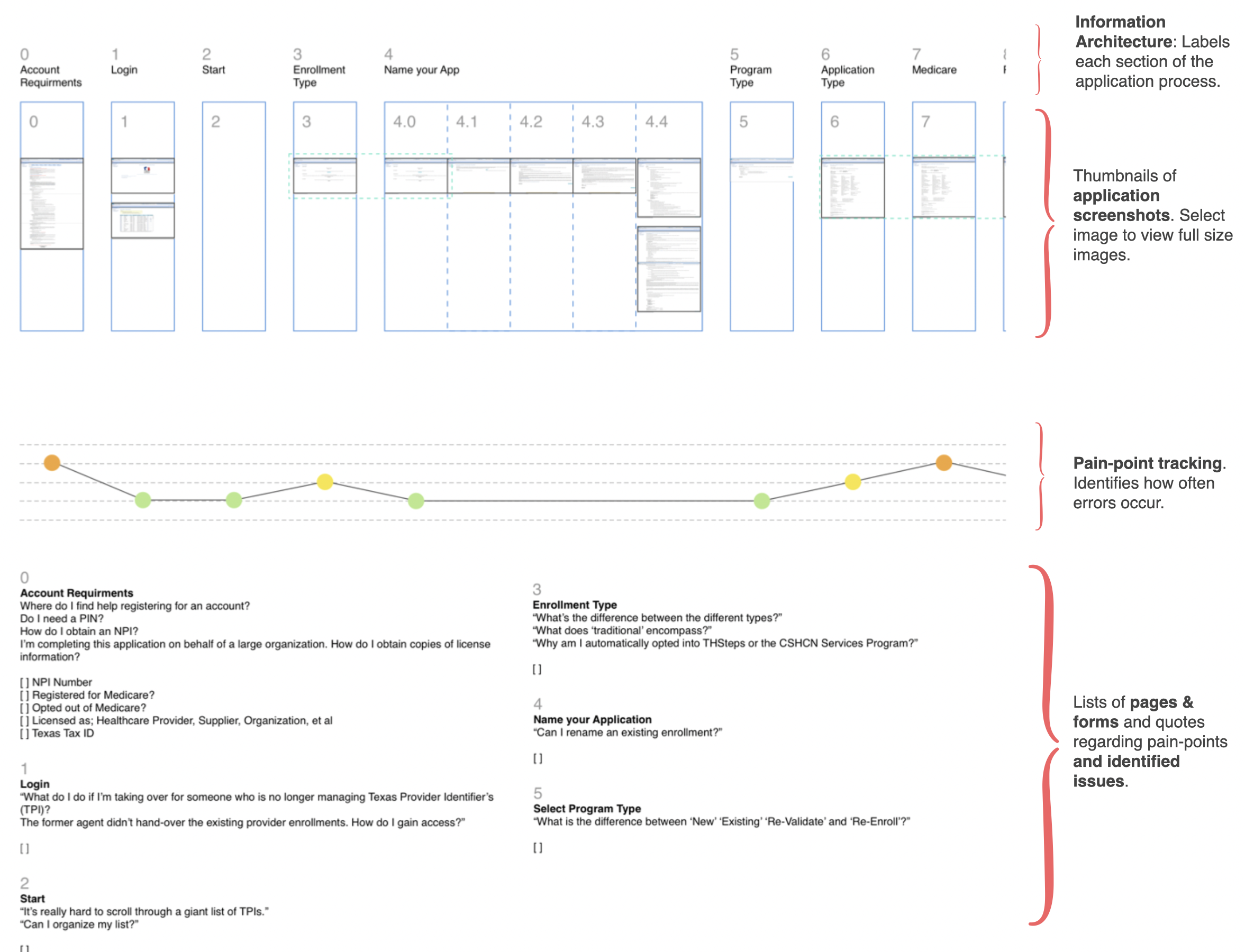
Operational KPI Analysis (Quantitative)
In addition to qualitative field research, this engagement incorporated quantitative analysis of operational performance data maintained by TMHP contractors (Accenture).
Method: Human KPI & Performance Data Analysis
I analyzed human performance metrics used by TMHP processing specialists to monitor enrollment throughput and support operations. These KPIs were not part of an automated analytics system; they were maintained through internal tracking tools and spreadsheets and reflected the realities of a legacy, paper-based workflow.
The metrics reviewed included:
Contact center resolution time
Volume and frequency of application rework
Application rejection and resubmission rates
Escalation patterns between processors and call center agents
Time-to-enrollment delays attributable to form errors or policy misinterpretation
These quantitative signals were used to:
Identify systemic bottlenecks rather than isolated usability issues
Correlate observed qualitative pain points with measurable operational impact
Validate where content ambiguity and process breakdowns were driving rework and escalation
Establish a baseline for improvement against which near-term recommendations could be evaluated
Because the data were manually entered and operationally constrained, the analysis focused on trend direction and pattern consistency rather than statistical precision. This approach was appropriate to the system’s maturity and avoided overconfidence in noisy or incomplete data.
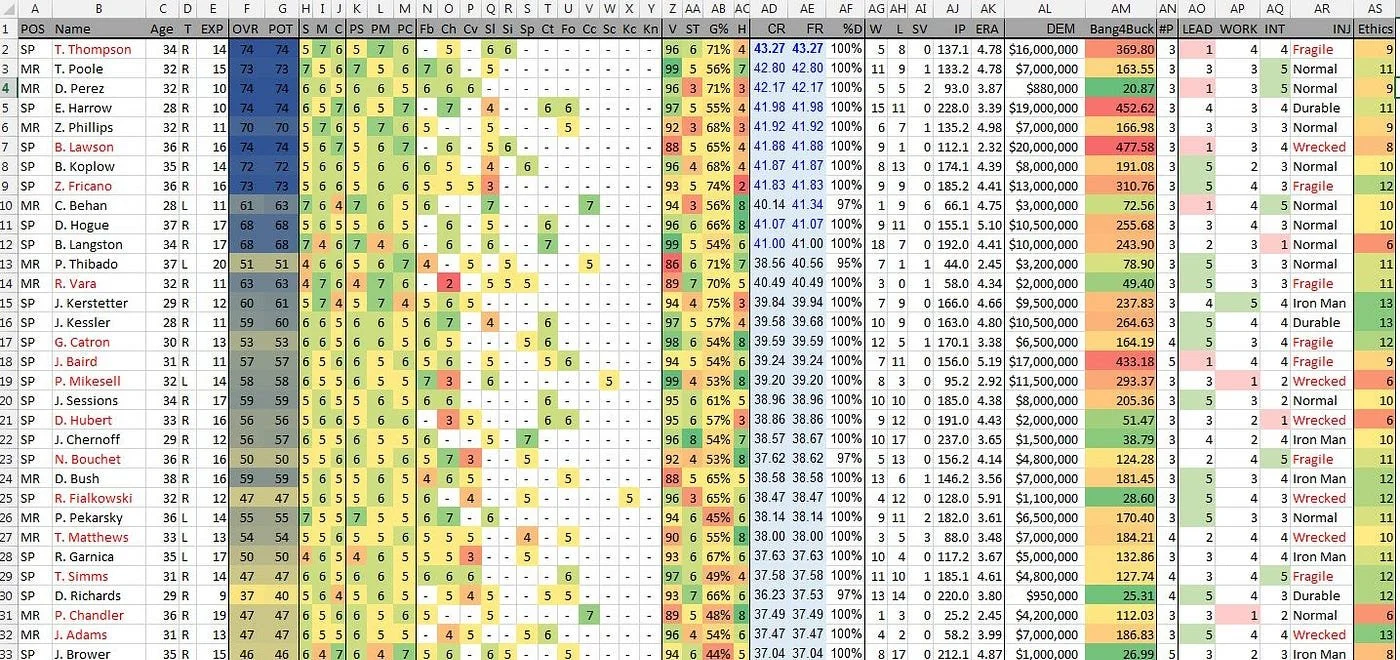
Note: This image is illustrative and does not contain real project data. It is included to convey the sophistication of the data analyzed during the engagement.
Design Artifacts
Rather than proposing a full system overhaul, I designed intermediate artifacts that addressed immediate pain while enabling long-term evolution.
Artifact 1: Content Governance Framework (Foundation for Automation)
I proposed and initiated a content governance program that included:
a full inventory of public- and staff-facing content
ownership and review cycles aligned to policy changes
plain-language and UX writing standards
lightweight version control to prevent drift
a shared knowledge base structure for processors and call center agents
I also designed an information architecture and taxonomy that:
classified content by task, provider type, and policy area
enabled modular reuse across channels
supported future AI-powered retrieval and assistance TX Medicaid Provider Enrollment…
This reframed IA as infrastructure, not navigation.
Artifact 2: Guided Support Tool (Logic-Based Decision Support)
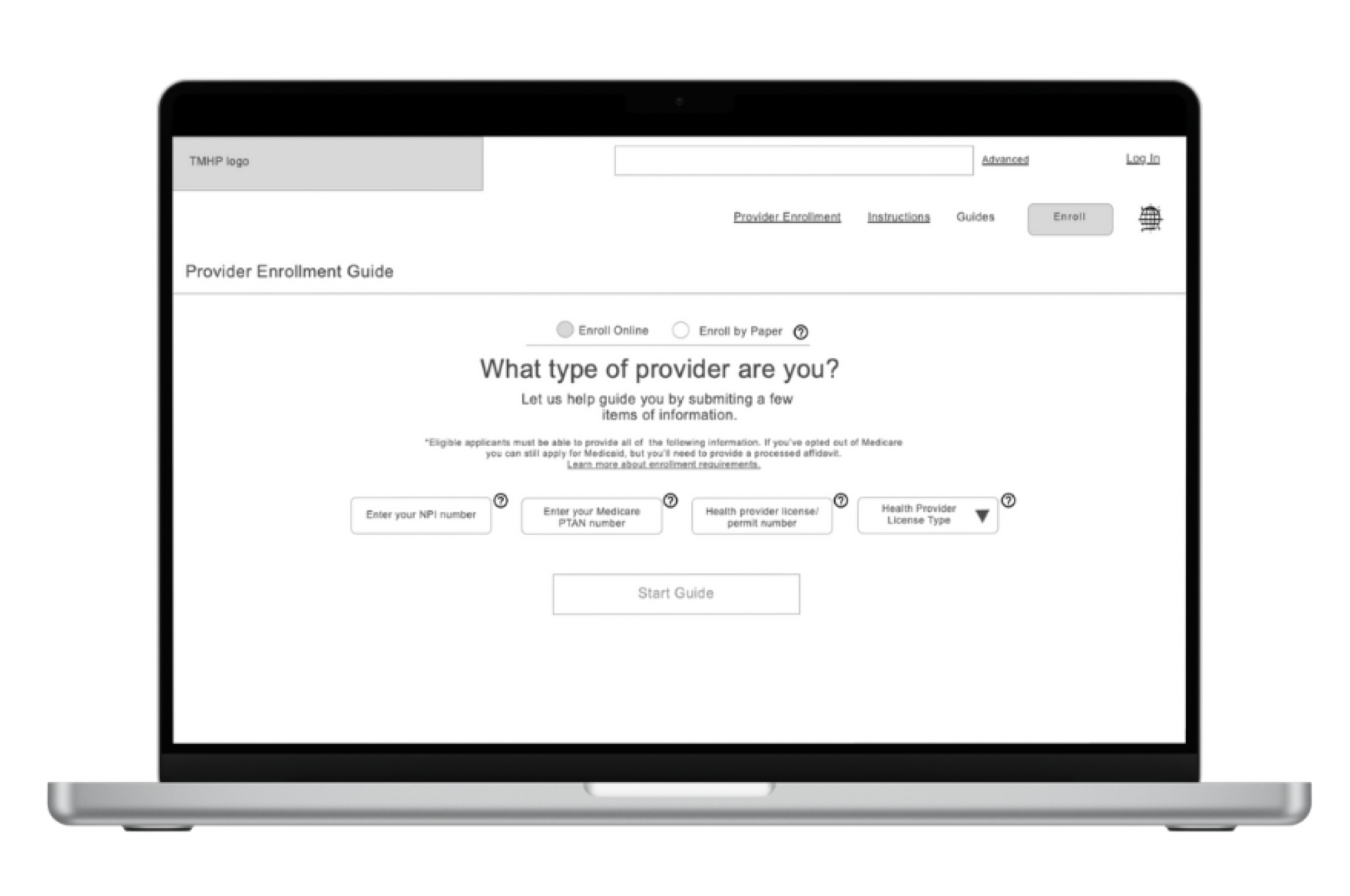
To reduce errors before they enter the system, I designed and prototyped a guided support tool that:
asked providers a series of simple, logic-based questions
dynamically narrowed the scope of required forms and steps
produced a customized enrollment guide with only relevant content
reduced cognitive load and ambiguity at the point of submission
Example questions included:
What type of provider are you?
Will you bill Medicaid directly?
Are you part of a group practice?
The tool demonstrated how low-tech decision support could dramatically reduce error even within a paper-based system.
Core Insight
The most important finding was that many errors were not workflow failures, but content failures.
Inconsistent, outdated, and poorly governed content:
caused providers to submit incorrect applications
forced processors to rely on informal interpretations
drove repeated call center escalations
created cascading rework loops that no amount of training could fix TX Medicaid Provider Enrollment…
This reframed the problem:
Content was not a usability issue — it was a systemic blocker to transformation.
Without structured, governed, and policy-aligned content, neither efficiency nor automation was possible.
Evaluation & Outcomes
Although this was not a full system replacement, the interventions produced measurable impact:
Results
28% reduction in contact center resolution time
Decreased rework and application rejections
Improved provider confidence and processor efficiency
Strengthened alignment across policy, processing, and design
Established a foundation for scalable, AI-enabled knowledge systems TX Medicaid Provider Enrollment…
Feedback from providers and processors confirmed:
improved clarity
reduced uncertainty
increased confidence during submission
less reliance on call center escalation
Design Science Contribution
This project demonstrates several key design science contributions:
Constraint-Driven Innovation
Meaningful transformation can occur without ideal conditions if design focuses on structural leverage points.Content as System Infrastructure
Governed, modular, policy-aligned content is a prerequisite for automation — not a downstream optimization.Design as Knowledge Production
The artifacts produced (governance model, IA, guided tool) functioned as theory-in-use, not just deliverables.Human-Centered Foundations for AI
AI-ready systems begin with clarity, structure, and governance — not models.
What I Learned
This project reinforced a core principle of my design practice:
Transformation doesn’t require perfect systems — it requires clarity, collaboration, and artifacts that respect reality while preparing for the future.
By designing within constraints rather than around them, we moved an outdated public-sector process forward one deliberate step at a time — with impact that extended well beyond the immediate intervention